Abstract
There are several reasons why investigators are interested in assessing visual function in children:
- Visual function is generally underdeveloped in new-borns and thus its development needs to be characterised.
- Knowledge of typical visual development allows clinicians to detect departures from the norm and intervene as soon as these are detected.
- Phenotype and onset of many cone-rod dystrophies is still unknown, generating an urgent need to characterise these conditions in the early years of life.
- Recent clinical trials are testing the theory that early intervention might be more successful in stopping the progression of a disease or restoring vision. This has lowered the recruiting age of the cohort to school-age children.
Ideally, to obtain consistent measurements, investigators should use the same test across all ages. This means that stimuli (for example, optotypes) and parameters (for example, light levels) used in the tests should be as similar as possible. Also, given the changes in attention span and ability to understand the test instructions, the tasks required by the tests should be as easy as possible and the overall assessment should be brief.
Metropsis offers a full battery of psychophysical tests that can be performed by adults as well as children from the age of 5. It has been shown that typically developing children falling into this age category are capable of performing simple tasks, such as choosing one alternative among few; have a relatively sustained attention span; are able to ask questions if the instructions are unclear and can be committed to complete challenging tasks. All these factors contribute to collecting reliable measurements.
On request, Metropsis can even include special techniques like preferential looking or habituation; these methods can extend the assessment to infants and preschool children, who are unable to use standard techniques due to restrictions related to language, physical or cognitive abilities. Furthermore, Metropsis can be extended with custom-developed, game-like tests, to help engage less compliant observers.
Keywords: visual development, visual acuity, visual function, spatial contrast sensitivity function, temporal contrast sensitivity function, grating acuity, ETDRS charts, Landolt C, Landolt ring, Sloan letters, myopia epidemiology, amblyopia, visual training, clinical treatment, visual rehabilitation, stereovision, stereo acuity, visual development, paediatric tests, random-dot stereograms, depth perception.
Jump to topic:
Visual Acuity
Why do I need to measure visual acuity in children?
- Monocular visual acuity assessment is a gold standard test for amblyopia; the visual acuity difference measured between the two eyes, is a strong indicator of amblyopia. This disease can affect between 1-2% of the paediatric population. Early detection of abnormal visual development may prevent a permanent impairment of visual function in the affected eye with a consequent loss of binocular vision.
- Visual acuity measurements are critical for the evaluation of refractive errors. Given the rapid increase of the prevalence of myopia during adolescence, the number of studies aiming to understand the causes of the myopia epidemiology has increased. For this reason, many government organisations have started to introduce visual screening in schools.
- Visual acuity is used as an index to monitor changes in visual function as a consequence of visual training or clinical intervention. In fact, several clinical trials aiming to treat genetic mutations causing rod-cone dystrophies, are now recruiting participants as young as 5.
How can I measure visual acuity in school-age children?
In infants and preschool children, behavioural visual acuity is typically investigated using preferential looking or habituation paradigms. Usually, the test stimuli consist of square-wave patterns and the measurement obtained is called grating acuity.
At birth, grating acuity is approximately 1/10th of that of adults, but it develops rapidly in the first year of life and it fully matures around the age of 51.
Typically developing school-age children can be tested with techniques and stimuli similar to those used with adults.
Metropsis offers a number of visual acuity tests suitable for assessing resolution acuity or recognition acuity. Resolution acuity measures the smallest spatial detail that can be resolved within a target. To do so, Metropsis uses the Landolt ring (aka Landolt C) to measure the smallest gap that the observer can resolve. The Landolt ring can be presented in isolation or surrounded by crowding bars, which make the test ideal for assessing visual acuity in amblyopic eyes.
Recognition acuity measures the correct identification of a target. To do so, Metropsis uses Sloan letters forming the Early Treatment of Diabetic Retinopathy Study (ETDRS) charts. Recognition acuity tests are more contingent to the child’s cognitive ability and communication skills.
Go to more information on the acuity tests available with Metropsis.
Contrast Sensitivity
Why do I need to measure contrast sensitivity function in children?
- Contrast sensitivity describes the sensitivity to contrast over a range of spatial frequencies, while visual acuity describes a single high-frequency cut-off point. According to Adams and Courage2, contrast sensitivity function is “the most complete single measure of human spatial vision” as it depicts vision and vision loss more completely than the single visual acuity measurement1. In fact, some visual disorders may selectively affect some spatial frequencies and not others, and thus could go unseen by the single visual acuity measurement. Conversely, contrast sensitivity measurements can detect disorders that affect visual acuity, as the visual acuity cut-off will be different from the normal cut-off.
- Spatial contrast sensitivity is often used for the assessment of amblyopia and as a measure of the influence of occlusion therapy or visual training.
- Contrast sensitivity tests are not limited to central vision and can be used to detect and monitor disorders that affect peripheral vision.
How can I measure spatial contrast sensitivity in school-age children?
There is general agreement that contrast sensitivity becomes adult-like somewhere between 7 years and 9-12 years. The figure below3 is an overview of the paediatric spatial contrast sensitivity development, as measured behaviourally.
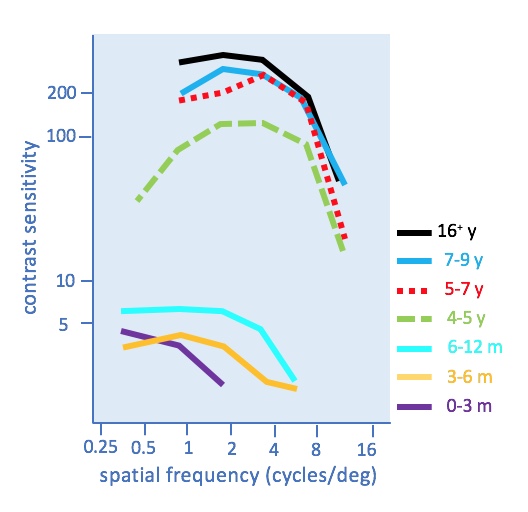
Contrast sensitivity for lower spatial frequencies (0.5 cpd) is present early in life, while sensitivity for higher spatial frequencies is still absent. After the first year, sensitivity to higher spatial frequencies develops very rapidly and reaches nearly adult-like levels by 4-5 years of age. Instead, sensitivity for lower spatial frequencies develops more slowly.
To obtain reliable psychophysical measurements, it is crucial that the contrast sensitivity test is administered using procedures that match the evolving cognitive abilities of the child and that the testing protocol is short and includes the possibility of breaks. When these requirements are met, school-age children can be assessed with the same methods used to test adults.
Metropsis allows the investigator to measure contrast sensitivity with different stimuli:
- Pelli-Robson charts
- Gabor stimuli
Go to more information on the spatial contrast sensitivity tests available with Metropsis.
Why do I need to measure temporal contrast sensitivity in children?
- The temporal sensitivity assessment allows investigators to characterise the visual response to rapid changes in light intensity. In some cone-rod dystrophies, this ability is severely compromised and thus its assessment is crucial to detect the onset and the progression that may take place after a clinical intervention.
- Temporal response is primarily driven by the magnocellular pathway. Some scientists argue that certain cases of dyslexia may be explained by a deficit of this pathway.
How can I measure temporal contrast sensitivity in school-age children?
One way to assess temporal vision is to assess the sensitivity to contrast (i.e. modulation depth) as a function of time. This can be achieved by presenting stimuli that vary sinusoidally over time; it is like presenting a grating pattern in time instead of space. The sensitivity to temporally modulated stimuli depends on their temporal frequency, amount of contrast, size of the stimuli and retinal location being stimulated. The visibility of temporal stimuli also seems to be contingent on age and degenerative disease.
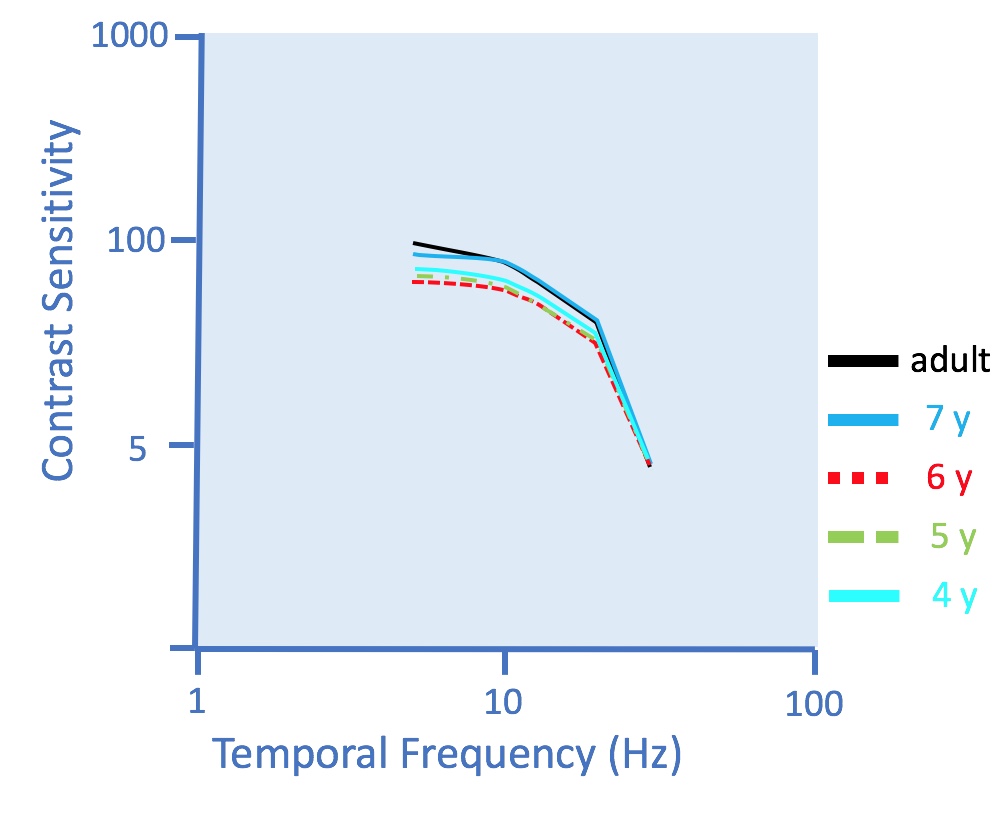
According to Ellemberg et al.4 there are different developmental patterns for spatial and temporal vision and for lower and higher frequencies. In particular, the critical flicker fusion frequency approximates adult-like around 3 months. This is achieved before sensitivity to lower temporal frequencies, grating acuity or sensitivity to lower spatial frequencies can match adult performance. In fact, it is only after age 6 that sensitivity to lower temporal frequencies become adult-like, as illustrated in Figure 2 below (re-drawn from Ellemberg et al. 1999).
The Metropsis flicker test presents a temporally modulated homogeneous blob to the left- or to the right-hand side of a fixation cross. The observer’s task is to respond whether the blob appears to the left or to the right by pressing either of two keys on a response box. This task is simple enough even for 5-year old children. The test is relatively short and can be further customised to accommodate less compliant observers.
Go to more information about the Metropsis flicker test.
Colour Vision
Why do I need to measure colour vision in children?
- Colour vision is the ability to distinguish lights only on the basis of their chromatic difference. This ability is severely compromised in subjects affected by genetic or acquired conditions which may affect one or more cone-classes. For example, about 8-10% of the male population is affected by protanomaly or deuteranomaly, which are defects associated with L-cones and M-cones respectively. Being unable to distinguish colours can affect children’s ability to read printed information.
- The assessment of colour vision is also used to identify brain tumours.
How can I measure colour vision in school-age children?
Like other visual functions, colour vision develops with age. Early studies by Davida Teller5 show that 2-month old infants can discriminate lights on the basis of their wavelength composition; however, discrimination along the Tritan axis seems less developed. When assessed psychophysically, children show higher chromatic discrimination thresholds than adults, as illustrated in the figure below, but there is no unanimous consensus on what is causing this difference.
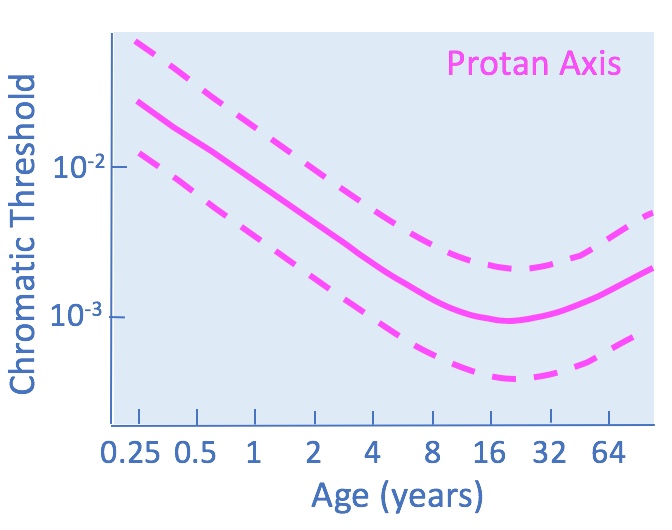
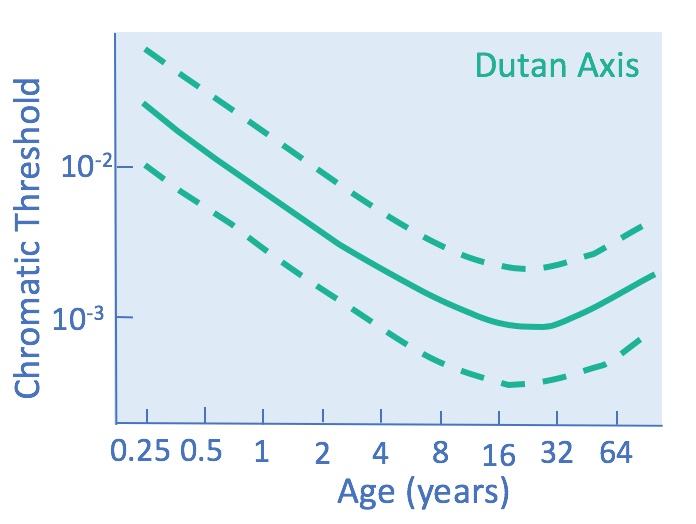
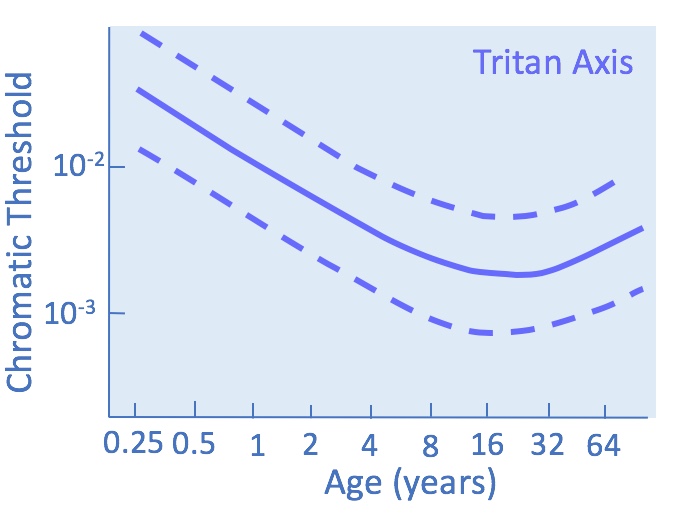
Figure 3. Colour discrimination thresholds along the Protan Deutan and Tritan confusion axes.
Undoubtedly, anatomical and functional changes are among the contributors. However, it has been suggested that the discrepancy may also be caused by the difficulty in performing the task required by the colour vision test, rather than the discrimination ability per se6.
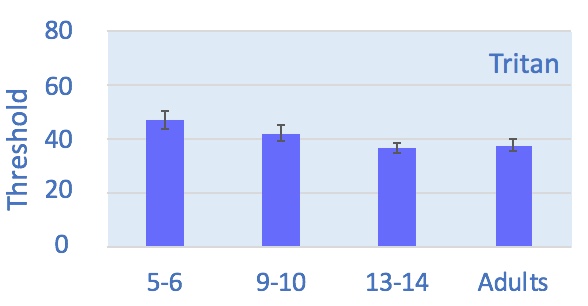
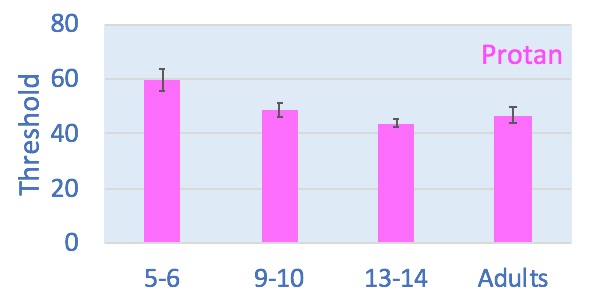
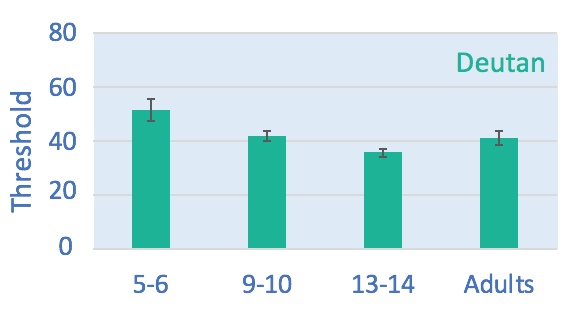
For example, the serial arrangement of the colour caps requested by the Farnsworth-Munsell 100-Hue Test seems to be an operation cognitively premature for some young children. When assessed with this test, children reach adult-like performance only around 13-14 years of age, as illustrated in figure 4 below.

Conversely, when the colour vision tests are based on different procedures (such as choosing an alternative among few possibilities) children as young as 9 reach adult-like performance, as shown in figure 5 below.
Metropsis offers three different computerised colour vision tests, all suitable for observers as your as 5. They are: Cambridge Colour Test (CCT), Low Vision Version of the CCT and Universal Colour Discrimination Test.
Each test can be run as quick screening or full assessment, according to the purpose of the test, the compliance of the observer and the time available.
Go to more information about the Metropsis colour vision tests.
Advantages of Metropsis
Why is Metropsis better than other commercially available visual assessment units?
- Metropsis tests are very easy to perform and thus can be use with children and young as 5; these tests are also suitable for adults. Using the same tests across different ages increases the reliability of measurements.
- Metropsis tests are generally quick to perform and their duration can be customised to optimise observer’s compliance.
- The tests are cognitively simple for observers to understand.
- The tests require very little training of the operator.
- Contrary to printed charts, (i) electronic charts do not degrade over time; (ii) the stimuli are randomly interleaved; (iii) scoring is recorded automatically, which reduces operator’s error or bias.
- Metropsis allows investigators to perform screening for visual conditions, or monitor subtle changes in visual function, for example: due to the onset of a disease or changes caused by clinical treatments or visual rehabilitation.
References
1Leat SJ, Yadav NK, Irving EL. Development of visual acuity and contrast sensitivity in children. J Optom 2009; 2: 19–26.
2Adams RJ, Courage ML. Using a single test to measure human contrast sensitivity from early childhood to maturity. Vision Res. 2002; 42:1205- 1210.
3Redrawn from Gwiazda J, Bauer J, Thorn F, and Held R. Development of spatial contrast sensitivity from infancy to adulthood: psychophysical data. Optom. Vis. Sci. 1997; 74: 785–789.
4Ellemberg D, Lewis TL, Liu CH, Maurer D, Development of spatial and temporal vision during childhood, Vision Res. 2002; 39: 2325–2333.
5Teller DY, Peeples DR, Sekel M. Discrimination of chromatic from white light by two-month-old human infants. Vision Res. 1978; 18:41 – 8.
6Ripamonti C, Kalwarowsky S, Nardini M, Investigative Ophthalmology & Visual Science 2015; 56: 4395.